
TL;DR:
- Enamel remineralization is a natural process where minerals are redeposited into weakened enamel, improving resistance to acid attacks. It is most effective on early lesions before cavities form, relying on factors like fluoride, saliva, diet, and oral pH to support mineral rebuilding. Consistent daily behaviors and innovative products help maximize remineralization, emphasizing prevention over restoration.
Tooth enamel is the hardest substance your body produces, yet it sits in a constant chemical battle every single day. Here’s the part most people get wrong: enamel remineralization is the natural process where minerals are redeposited into weakened enamel, making it more resistant to future acid attack. That means early damage can often be reversed, but once a real cavity forms, no amount of remineralization will restore what’s gone. Understanding this distinction changes how you approach your entire oral care routine.
Table of Contents
- What is enamel remineralization?
- How does the enamel remineralization process work?
- Which ingredients and technologies support remineralization?
- When does remineralization work—and when doesn’t it?
- How to support your enamel at home
- Why most people misunderstand enamel remineralization
- Take charge of your enamel health
- Frequently asked questions
Key Takeaways
| Point | Details |
|---|---|
| Enamel can be strengthened | Remineralization can reverse early enamel damage by restoring vital minerals. |
| Fluoride and minerals matter | Ingredients like fluoride, calcium, and phosphate help protect and reinforce enamel. |
| Home care is essential | Consistent oral hygiene and diet choices make a real difference. |
| Limits to reversal | Remineralization cannot regrow lost enamel or fix cavities; it is preventive, not restorative. |
| Clinical results vary | Effectiveness depends on the approach, daily habits, and your unique oral chemistry. |
What is enamel remineralization?
Enamel is the thin, semi-translucent outer shell covering every tooth. It contains no living cells, which is why your body cannot simply “grow it back” the way it heals a cut. What it can do is repair mineral loss at the microscopic level, provided the damage hasn’t gone too far.
Enamel remineralization is the natural process where minerals are redeposited into weakened or early demineralized enamel, strengthening it and making it more resistant to acid attack. Think of enamel’s crystal structure like a brick wall. Acid attacks chip away individual bricks. Remineralization sends replacement bricks back into those gaps, but only if the gaps haven’t collapsed the entire wall.
Understanding the key players helps put everything in context:
- Calcium and phosphate are the primary minerals that make up hydroxyapatite, enamel’s structural compound
- Fluoride acts as a catalyst, helping calcium and phosphate bond into the enamel lattice faster and creating a more acid-resistant form of mineral called fluorapatite
- Saliva is your mouth’s natural mineral delivery vehicle, constantly ferrying these ions to areas that need repair
- Oral pH determines whether the environment favors breakdown or rebuilding
“Enamel remineralization is the natural (mostly acellular) process where minerals are redeposited into weakened or early demineralized enamel, strengthening it and making it more resistant to future acid attack.”
This process is not a one-time event. It happens constantly, every hour you’re awake and eating. The science of minerals in oral care shows just how dynamic this equilibrium really is, and why your daily choices push it in one direction or the other.
How does the enamel remineralization process work?
Now that we know what remineralization means, let’s see how the process plays out in your mouth every day. The cycle is elegant in its simplicity, but the details matter a lot.
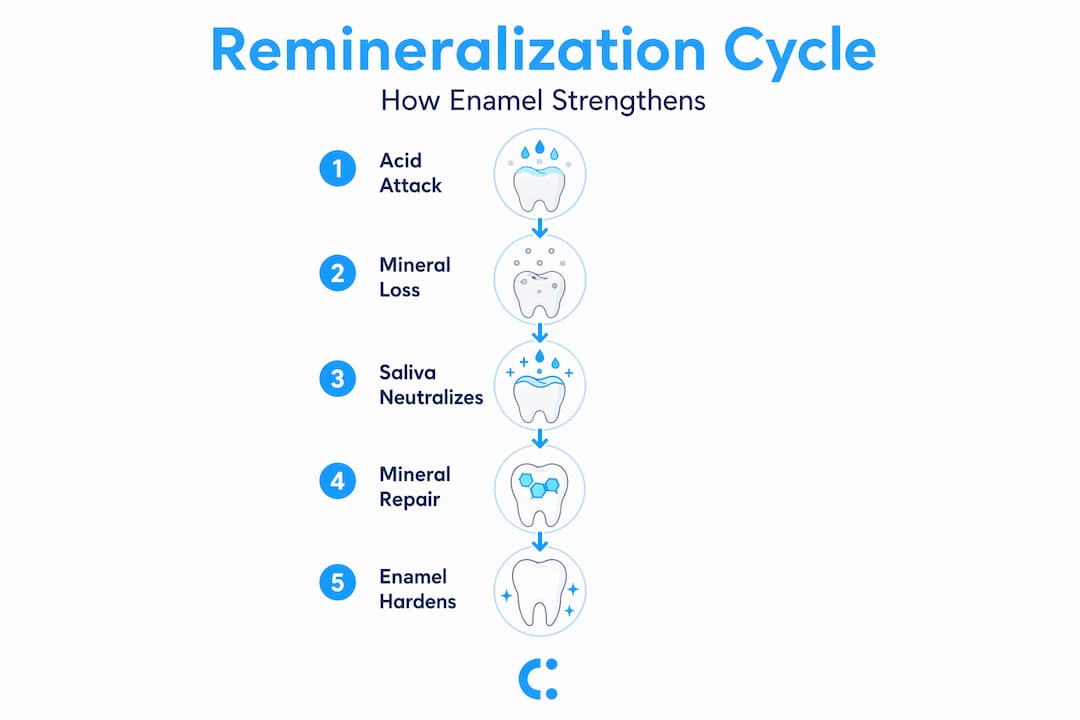
When you eat or drink something acidic, bacteria in your mouth also produce acids as a metabolic byproduct. Those acids lower the oral pH. When pH drops below 5.5, the acid environment pulls calcium and phosphate ions out of the enamel crystal lattice. This is demineralization, and it begins within minutes of acid exposure.

The driving mechanism in the mouth is a cycle: acids cause demineralization, and when the oral environment becomes less acidic, mineral ions in saliva can precipitate back into enamel’s crystal structure. Your saliva is what rescues you. It buffers the acid, raises the pH, and reintroduces the minerals needed to patch the lattice.
Here’s a side-by-side look at what pushes the cycle in each direction:
| Factor | Drives demineralization | Drives remineralization |
|---|---|---|
| Diet | Frequent sugary or acidic foods | Calcium-rich foods, water |
| Saliva | Low flow (dry mouth) | Healthy flow, buffering capacity |
| Oral pH | Below 5.5 | Above 5.5, ideally neutral |
| Fluoride exposure | None | Regular toothpaste or rinse use |
| Bacterial load | High (poor hygiene) | Low (consistent brushing, flossing) |
| Hydration | Dehydrated | Well hydrated |
To give remineralization its best chance, you need to:
- Reduce the frequency of acid exposure (not just the amount)
- Keep saliva flow healthy through hydration and chewing
- Maintain fluoride contact through toothpaste or rinses
- Give your mouth recovery time between eating events
- Manage bacterial populations with consistent brushing and flossing
Understanding oral minerals and enamel chemistry helps you see why snacking constantly throughout the day is so destructive. Each snack resets the acid clock, cutting into the recovery window your saliva needs. You can also learn more about how to optimize dental chemistry with targeted daily habits.
Pro Tip: Wait at least 30 minutes after eating before brushing. Brushing immediately after an acid challenge can physically remove softened, demineralized enamel before saliva has had a chance to begin re-hardening it.
Which ingredients and technologies support remineralization?
With the process in mind, let’s look at what actually helps your teeth reabsorb minerals. The ingredient space has gotten significantly more sophisticated over the past decade, and not all agents work the same way.
Fluoride remains the most studied and widely recommended remineralization agent in clinical dentistry. Fluoride supports remineralization primarily through topical effects and can enhance formation of more acid-resistant mineral, specifically fluorapatite, which is harder and less soluble than the original hydroxyapatite. This is why fluoride toothpaste isn’t just a cavity preventative. It actively changes the chemistry of enamel so future acid attacks do less damage.
CPP-ACP (casein phosphopeptide-amorphous calcium phosphate) is a milk-derived protein complex that acts as a reservoir of bioavailable calcium and phosphate. It binds to tooth surfaces and delivers ions directly where they’re needed. Research shows it’s particularly effective in people with low salivary flow, where the natural mineral delivery system is compromised.
Nano-hydroxyapatite is a biomimetic (meaning it mimics biological structures) form of the same mineral that makes up enamel. At the nanoscale, particles are small enough to physically integrate into the enamel surface. Biomimetic remineralization approaches including nano-hydroxyapatite have been evaluated extensively in lab and in situ studies, with reported efficacy varying by model and endpoints.
Here’s a quick data comparison across the three leading agents:
| Agent | Primary mechanism | Acid resistance | Availability | Best for |
|---|---|---|---|---|
| Fluoride | Fluorapatite formation | High | Toothpaste, rinses | Broad prevention |
| CPP-ACP | Ion reservoir delivery | Moderate | Specialty pastes, chews | Dry mouth, high-risk patients |
| Nano-hydroxyapatite | Biomimetic integration | Moderate to high | Premium toothpastes | Sensitivity, early white spots |
Clinical evidence suggests remineralization protocols can reduce progression and lesion signals around enamel defects over months, with measurable differences among agents. This is meaningful data, particularly for people in orthodontic treatment where white spot lesions around brackets are a real risk.
Pro Tip: If you’re evaluating remineralization products, look past the marketing and check the active ingredient list. Products claiming to “restore enamel” with only abrasive particles and no actual remineralization agents are selling surface polish, not structural repair.
Understanding how minerals strengthen enamel at the structural level makes it much easier to read these ingredient lists with a critical eye and choose products that actually deliver on their claims.
When does remineralization work—and when doesn’t it?
It’s important to set realistic expectations about what remineralization can and can’t do. This is where a lot of consumer confusion, and frankly a lot of product marketing, runs off the rails.
Remineralization works on early lesions. These are areas where the enamel surface is still mostly intact but the subsurface has lost mineral density. You often can’t see these with the naked eye, but your dentist may identify them as white spot lesions or early demineralization zones. When caught at this stage, consistent remineralization therapy can genuinely reverse the process and prevent the lesion from progressing to a cavity.
Here’s what actually falls within the scope of remineralization:
- Early white spot lesions on the enamel surface
- Subclinical mineral loss not yet visible as a structural defect
- Increased surface roughness from acid erosion before physical enamel loss occurs
- Sensitivity reduction through partial occlusion of exposed dentinal tubules
“Remineralization can help with non-cavitated or early enamel lesions, but it cannot restore enamel once it is destroyed, for example, when a cavity has formed.”
Once the enamel structure physically breaks down, creating a cavitation, or hole, the cavity cannot be mineralized back into solid tooth structure. The structural scaffold is gone. At that point, professional dental treatment is the only path forward. No toothpaste, no chewing gum, and no rinse will fill that space with new enamel.
The importance of minerals for enamel is greatest before a cavity forms. The window for remineralization is real, but it’s not unlimited. This makes early detection and consistent preventive care critically important.
How to support your enamel at home
If you want stronger enamel, here’s what you can actually do day-to-day. The science is clear that creating conditions for remineralization hinges on reducing repeated acid challenges, maintaining fluoride exposure, and maintaining a healthy saliva environment. That translates into specific, repeatable behaviors.
- Limit acidic food and drink frequency. The number of acid exposures per day matters more than total quantity. Three sodas at lunch is better than one soda sipped over three hours.
- Brush with fluoride toothpaste twice daily. Use a soft bristle brush and a pea-sized amount. The fluoride needs contact time with enamel to work effectively.
- Stay hydrated throughout the day. Saliva needs water to flow. Chronic dehydration means chronic under-delivery of remineralizing minerals.
- Chew sugar-free gum after meals. Chewing stimulates saliva production, raises oral pH faster, and helps flush food debris. This is particularly effective in the 20-minute window after eating.
- Eat calcium and phosphate-rich foods. Dairy, leafy greens, eggs, nuts, and legumes all contribute to the mineral pool your saliva draws from.
- Use a fluoride mouth rinse before bed. This extends fluoride contact time overnight when saliva flow naturally decreases.
- See your dentist regularly. Professional cleanings remove calculus that home care can’t, and early lesion detection keeps you in the remineralizable window.
The role of minerals and daily enamel care is cumulative. No single action reverses enamel damage, but sustained daily behavior shifts the balance meaningfully toward repair. You can also explore natural dental health methods that complement your routine without adding complexity.
Pro Tip: Rinse with plain water immediately after consuming acidic foods or drinks. It takes seconds, costs nothing, and rapidly begins raising your oral pH back toward the safe zone above 5.5.
Why most people misunderstand enamel remineralization
Let’s step back and make sense of what all this really means for consumers. The frustrating truth is that the oral care market has overloaded the word “remineralization” to the point where it has nearly lost meaning.
Here’s the uncomfortable reality: most research on remineralization is conducted using artificial saliva and controlled pH-cycling in laboratory conditions. Real-world remineralization results often fall short of laboratory data because lab models lack the variables of actual chewing, biofilm complexity, diet variation, and unpredictable oral pH swings that define real life. A product that achieves impressive remineralization in a pH-cycling study may perform significantly differently in your mouth over six months.
This doesn’t mean remineralization is a myth. It means it’s subtle, slow, and fundamentally preventative rather than restorative. Most clinical improvements show up over months of consistent effort, not weeks of trying a new toothpaste. The people who see the best real-world results are those who stack multiple favorable behaviors, diet changes, fluoride exposure, hydration, and chewing stimulus rather than relying on any single product.
We also think there’s a delivery problem that doesn’t get enough attention. A remineralizing agent sitting in a tube does nothing until it reaches your enamel surface and stays there long enough to work. Products that actively stimulate saliva and prolong contact time in the oral environment have a structural advantage because the mouth itself becomes the delivery mechanism. That’s a fundamentally different approach than passive paste application. Exploring improving dental health naturally shows how behavioral and product-based strategies can work together more effectively than either alone.
The bottom line from our perspective: treat remineralization as a daily infrastructure investment, not a repair job. The best version of your enamel health comes from never letting demineralization win consistently in the first place.
Take charge of your enamel health
Ready to support your enamel? Here’s a smart place to start.
Everything you’ve read here points in one direction: the window for real remineralization is open, but daily consistency is what keeps it open. Products that work with your mouth’s biology, stimulating saliva, delivering minerals, and supporting the right oral chemistry, give you a meaningful edge over passive care alone.
Scandigum is engineered specifically around this logic. Each piece of gum stimulates salivary flow, introduces mineralizing support, and leverages the buccal environment to shift your oral chemistry toward active repair rather than passive decay. If you’re serious about protecting your enamel from the inside out, Scandi Gum enamel care is designed to fit right into your existing routine as a functional upgrade, not an afterthought. Your enamel doesn’t get a second chance once it’s truly gone. Give it the best daily environment you can.
Frequently asked questions
Can you regrow tooth enamel once it is lost?
No. Once enamel is lost to a cavity or significant erosion, it cannot regrow. Remineralization only addresses early, non-cavitated enamel damage before structural collapse occurs.
Does remineralization toothpaste really work?
Yes, when used consistently and when the product contains proven active agents. Fluoride, CPP-ACP, and nano-hydroxyapatite are the leading remineralization agents with documented clinical and laboratory effects on early enamel lesions.
What foods help remineralize tooth enamel?
Dairy products, leafy greens, nuts, eggs, and legumes are rich in calcium and phosphate, the two minerals your saliva draws on to redeposit into enamel during the natural remineralization cycle.
How long does enamel remineralization take?
Minor early lesions may show measurable improvement over several months of consistent care. Results depend on lesion severity, the remineralization agents used, and how well daily behaviors support a favorable oral environment.
Is drinking water important for remineralization?
Yes. Hydration supports healthy saliva production, which is the body’s primary vehicle for delivering calcium, phosphate, and buffering capacity to enamel surfaces throughout the day.