
TL;DR:
- Many supplements have low oral bioavailability, meaning only a small fraction of ingested compounds reach the bloodstream in active form. Choosing delivery formats like liposomes, buccal, or sublingual options can vastly improve absorption and efficacy. Prioritizing bioavailability data over milligram counts enables smarter supplement decisions that better support health and performance.
You take your supplement, swallow the capsule, and assume the 500 mg on the label is what your body receives. It isn’t. Oral bioavailability is the fraction of an orally administered substance that actually reaches your bloodstream in an active, usable form, and for many common supplements, that fraction is shockingly small. The milligram count on a bottle tells you what went in, not what got through. Understanding this single concept will permanently change how you evaluate every supplement, energy product, and oral health formula you consider buying.
Table of Contents
- What is oral bioavailability and why does it matter?
- How oral bioavailability is measured: The science simplified
- What lowers oral bioavailability? The hidden obstacles
- How to improve oral bioavailability: Strategies for smarter absorption
- Why most consumers miss the point on oral bioavailability
- Enhance your wellness with smarter delivery
- Frequently asked questions
Key Takeaways
| Point | Details |
|---|---|
| Absorption over dosage | The amount your body actually uses matters more than the supplement’s label dosage. |
| Barriers reduce efficacy | Gut, liver, and digestive enzymes lower how much of an oral product enters your bloodstream. |
| Optimize delivery methods | Choosing advanced formulations and smart pairing can boost your supplement’s bioavailability. |
| Be label-savvy | Read supplement labels for evidence of improved absorption, not just high milligrams. |
What is oral bioavailability and why does it matter?
Think of oral bioavailability as your body’s “efficiency rating” for any substance you swallow. Scientists use the letter F to represent it, and it’s expressed as a percentage. An F of 100% means every milligram you consume reaches your blood circulation unchanged and ready to work. An F of 20% means four out of every five milligrams never make it.
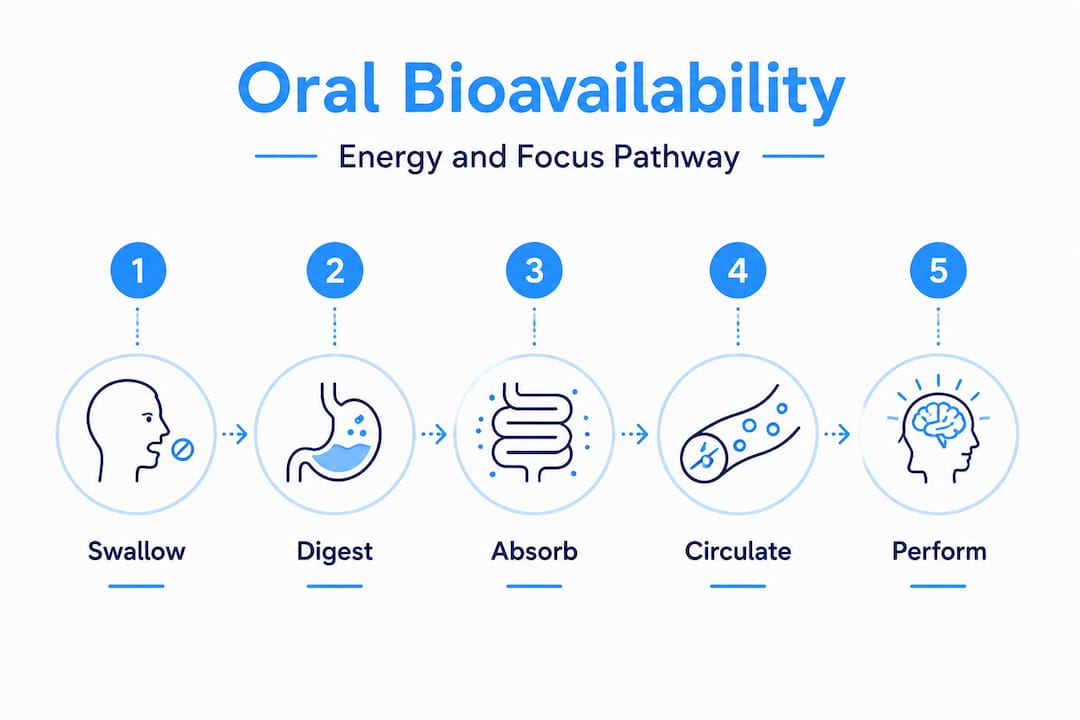
Why does only a portion get through? Because the route from your mouth to your bloodstream is long and full of biological checkpoints. Stomach acid can degrade a compound before it even reaches the intestine. Gut-wall enzymes can break it down further. Then the liver applies what pharmacologists call “first-pass metabolism,” converting or neutralizing a significant chunk of what remains before it enters general circulation. Each stage chips away at the amount your tissues actually receive.
The real-world impact on energy, focus, and health is direct:
- A caffeine formula with 85% bioavailability delivers noticeably more active caffeine to your brain than a competing product with 50% bioavailability at the same labeled dose.
- An iron supplement taken without the right cofactors may reach a bioavailability as low as 2%, making that “high-potency” label essentially meaningless.
- B vitamins absorbed sublingually (under the tongue) or buccally (through the cheek lining) skip several degradation steps and reach the bloodstream faster and in higher concentrations.
“Oral bioavailability is the fraction (percentage) of an orally administered substance that reaches systemic circulation in an active, unmodified form, and it is what determines a product’s true functional dose.”
The contrast between high dose, low absorption and lower dose, high absorption is not academic. It determines whether a product actually changes how you feel. Choosing supplements based on oral delivery systems rather than raw milligram counts is the single most practical upgrade you can make to your supplement strategy. And once you understand how delivery and oral delivery and cognition are linked, the connection between absorption and mental performance becomes impossible to ignore.
How oral bioavailability is measured: The science simplified
Scientists needed a reliable benchmark to measure how much of a substance actually gets through to the bloodstream. Their solution: compare oral delivery to intravenous (IV) delivery, which bypasses every biological barrier entirely and is therefore defined as 100% bioavailability. Everything else is measured relative to that gold standard.
Here’s how absolute bioavailability is calculated, step by step:
- Administer the substance orally to a test subject and measure blood concentration at multiple time points.
- Plot those concentrations on a graph over time. The total area under that curve is called the AUC (area under the curve), and it represents total systemic exposure to the substance.
- Repeat the experiment with an IV dose of the same substance. This gives you a second AUC, normalized to the dose administered.
- Divide the oral AUC by the IV AUC (adjusted for any difference in doses). The result, expressed as a percentage, is absolute bioavailability (F).
This method removes guesswork. Instead of assuming that a 200 mg capsule delivers 200 mg of active compound, AUC-based measurement tells you exactly how much the body was exposed to, and for how long.
| Delivery method | Typical bioavailability range | Why it varies |
|---|---|---|
| Intravenous (IV) | 100% | No absorption barriers |
| Buccal / sublingual | 50–90% | Bypasses first-pass liver metabolism |
| Standard oral capsule | 10–60% | Subject to digestion and liver clearance |
| Enteric-coated tablet | 20–70% | Protected from stomach acid, variable gut uptake |
| Peptide supplement (oral) | Often less than 5% | Enzymatic degradation is severe |
As the absolute bioavailability formula confirms, the comparison of dose-normalized AUC values between oral and IV routes is the method pharmacologists rely on most. For everyday consumers, that means the delivery format of your supplement is as important as the ingredient list itself.
Pro Tip: When two products contain the same active ingredient, look for the one with clinical AUC data or third-party bioavailability testing rather than simply choosing the higher milligram count. A 100 mg dose with 80% bioavailability delivers more usable compound than a 300 mg dose with 20% bioavailability.
What lowers oral bioavailability? The hidden obstacles
Several distinct biological barriers stand between a swallowed supplement and your bloodstream. Overall oral bioavailability in pharmacokinetics is essentially the product of three sequential factors: how much is absorbed from the gut (Fa), how much survives the gut wall (Fg), and how much escapes liver metabolism without being deactivated (Fh). Multiply these three fractions together and you get F, your effective dose.

Fa: Absorption from the gut This is how well the intestinal lining physically takes up the compound. Fat-soluble nutrients generally absorb better than water-soluble ones in certain contexts. Particle size, solubility, and gut transit time all affect Fa. A supplement that dissolves slowly or clumps in the stomach may pass through without significant uptake.
Fg: Gut-wall metabolism The cells lining your small intestine contain enzymes, particularly the CYP3A4 enzyme family, that can chemically alter compounds before they even enter the portal bloodstream. Some substances lose 30 to 50% of their effective concentration right here, before the liver even sees them.
Fh: Hepatic first-pass effect The liver receives everything absorbed from your gut before it reaches general circulation. For many compounds, liver enzymes rapidly convert them into inactive metabolites. This is the hepatic first-pass effect, and it’s the reason oral morphine requires a much higher dose than an injected equivalent, and why some supplements designed for oral consumption deliver a fraction of their labeled potency.
| Supplement type | Estimated oral bioavailability | Primary bottleneck |
|---|---|---|
| Caffeine | 80–99% | Minimal first-pass; very efficient |
| Vitamin C | 70–90% at low doses | Saturable gut transport |
| Magnesium (oxide form) | 4–14% | Poor intestinal solubility |
| Curcumin (standard) | Less than 1% | Rapid gut and liver metabolism |
| Therapeutic peptides | Often less than 1% | Enzymatic degradation throughout |
| CoQ10 (standard) | 2–5% | Fat-solubility challenges |
Enzymatic degradation and transport barriers can keep oral bioavailability extremely low even in products specifically engineered for oral delivery. This isn’t a formulation failure; it’s basic biology doing exactly what it was designed to do, protecting your body from unknown ingested compounds.
Common factors that reduce oral bioavailability include:
- Low aqueous solubility of the active compound
- Rapid gut motility that moves the substance through before absorption completes
- High protein binding in the gut that ties up active molecules
- Competing dietary components that block absorption pathways (e.g., calcium interfering with iron)
- Unstable chemical structure that degrades under stomach acid conditions
- Efflux transporters in the gut wall that actively pump some compounds back out
“For many peptides and proteins, oral bioavailability can be below 1%, meaning 99 cents of every functional dollar you spend never reaches your biology.”
Understanding functional gum absorption as an alternative delivery pathway matters precisely because it sidesteps most of these barriers entirely, absorbing compounds through the buccal mucosa directly into the bloodstream before the gut and liver even get involved.
How to improve oral bioavailability: Strategies for smarter absorption
Knowing the obstacles is only useful if you know how to work around them. Here are actionable strategies that actually move the needle on how much of a supplement your body uses:
- Choose advanced delivery formats. Liposomal supplements encapsulate active compounds in fat-based vesicles that fuse directly with cell membranes, dramatically improving uptake. Enteric-coated capsules protect acid-sensitive compounds through the stomach. Buccal and sublingual formats skip the GI tract entirely.
- Pair fat-soluble nutrients with healthy fats. Vitamins D, E, K, and A and compounds like CoQ10 dissolve in fat. Taking them with a meal containing avocado, olive oil, or nuts can increase their absorption by two to five times compared to taking them on an empty stomach.
- Use black pepper extract (piperine) with curcumin. Piperine inhibits the enzymes that rapidly clear curcumin from the body. Studies show it can increase curcumin bioavailability by up to 2,000%, turning a near-useless oral dose into a functionally active one.
- Time your supplements around gut motility. Some compounds absorb better when gut transit is slower, typically after a meal. Others need an empty stomach to avoid competition with food components for absorption transporters.
- Prioritize formulation quality over raw milligrams. Better bioavailability means the formulation and delivery chemistry genuinely improve exposure to systemic circulation, reflected in measurable AUC values, rather than simply showing a larger number on the label.
Practical things to look for when comparing products:
- Clinical bioavailability data (AUC comparisons published or cited by the manufacturer)
- “Liposomal,” “nano-emulsified,” “enteric-coated,” or “buccal” on the label
- Bioenhancers listed as ingredients (piperine, quercetin, phosphatidylcholine)
- Formats that bypass the GI tract when the active ingredient is gut-unstable
Pro Tip: If a supplement’s label does not mention how the product addresses absorption or bioavailability, that silence is itself information. Brands that invest in delivery science talk about it because it differentiates them. Generic capsules without bioavailability data are often a bet on milligrams, not on results.
Exploring how minerals and absorption interact in oral care contexts reveals another dimension of this conversation. Even the minerals you expose your mouth to during chewing or oral care routines can influence local and systemic nutrient dynamics.
Why most consumers miss the point on oral bioavailability
Here’s the uncomfortable reality: the supplement industry built itself on a metric that is easy to print on a label, milligrams, rather than the metric that actually predicts results, bioavailability. And most consumers have never been told the difference.
Walk through any health store and you’ll hear people comparing products by “how many milligrams” they contain. The 1,000 mg bottle wins over the 400 mg bottle. Bigger feels better. It’s intuitive. It’s also frequently wrong.
The smartest health consumers we’ve observed don’t shop for dosage. They shop for delivery. They ask “what format is this in?” before they ask “how much does it contain?” They know that a 200 mg buccal dose of a well-absorbed compound can outperform a 1,000 mg capsule of the same compound delivered through standard oral ingestion, because the biology supports it.
There’s also a deeper issue. Many people have been disappointed by supplements that “didn’t work” and concluded the active ingredient was ineffective. Often, the ingredient itself was sound. The delivery was the failure. Curcumin doesn’t fail to reduce inflammation because it lacks potency at the molecular level. Standard curcumin capsules fail because less than 1% of the labeled dose survives to reach systemic circulation.
The challenge we’d put to you is this: before your next supplement purchase, find the bioavailability data. If it doesn’t exist, ask why. If the brand can’t provide it, that tells you something important. Rethinking absorption as the primary filter for supplement selection isn’t a minor upgrade to your routine. It’s a fundamental shift in how you respect your own biology and your own investment.
Enhance your wellness with smarter delivery
Most supplement strategies focus on what goes in, not what gets through. If the science in this article has shifted how you think about absorption, the next logical question is: which formats actually deliver?
Scandigum was built around that exact question. Rather than adding more milligrams to a standard capsule, the format itself is the technology. Functional gum leverages the buccal mucosa, the highly vascularized lining of your mouth, to move active compounds directly into your bloodstream, bypassing the GI tract and the liver’s first-pass clearance entirely. The result is faster onset, more predictable exposure, and a sustained “ledge” of energy and focus rather than a spike and crash. If you’re ready to invest in absorption rather than just milligrams, explore the Scandi Gum product page and see how delivery science translates into real, felt results.
Frequently asked questions
Why isn’t all of a supplement absorbed by the body?
Oral supplements lose significant portions of their active ingredients to stomach acid, gut-wall enzymes, and liver first-pass metabolism before they ever reach general circulation. The route from mouth to bloodstream has multiple checkpoints that reduce what finally gets through.
How can I tell if a product has high oral bioavailability?
Look for clinical AUC data, published absorption studies, or formulation technologies on the label such as “liposomal,” “enteric coated,” or “buccal delivery,” as these signal that the manufacturer has prioritized how well the compound actually reaches your system.
What substances struggle most with oral bioavailability?
Peptides, proteins, and poorly soluble compounds like curcumin typically have the lowest oral bioavailability because enzymatic degradation and transport barriers break them down before they can be absorbed into the bloodstream.
Does higher dosage always lead to better results?
No. Higher dosage does not guarantee better results when the body cannot efficiently absorb the active ingredient, because better bioavailability means optimizing systemic exposure through formulation science rather than simply increasing the labeled milligram count.